Pulling another article from the notebook archive, penned March 20, 2020.
I have seen the future of IV workflow management systems (IVWFMS). Spoiler alert, EPIC wins. And before people start calling me an Epic fanboy, I should make it clear that I do not like Epic, as a company or a product. I believe healthcare will rue the day they relinquished all their power to a single company.
Those that know me or have read anything I have written in the past decade, know that I am an advocate for technology in the IV room. People are imperfect creatures, they make mistakes. Don’t believe me? Google Emily Jerry death or St Charles rocuronium. That will tell you all you need to know about the dangers associated with injectable medications. Compounded sterile preparations are the most dangerous medications within the four walls of a hospital. Seems logical that such dangers would receive the utmost attention. Inexplicably, they do not. Many reasons are given for ignoring the issues, but it boils down to poor planning and the inability to prioritize in the face of budgetary and political restraints.
Technology, while far from perfect, adds a level of protection to a complex, error-prone, and dangerous process. Adding a little common-sense technology to the IV medication process, like an IVWFMS*, is the quickest and most cost-effective way to improve safety.
Implementing these systems is a no-brainer, but that hasn’t stopped people from ignoring them. The problem has been, at least from my perspective, a complete failure by pharmacy leadership to recognize and prioritize IV room safety and efficiency. Nowhere else but in the IV room can a single mistake result in significant harm or death. Yet the IV room seems to get a fraction of the attention it should. Unfortunately, it often takes a tragic error like those noted above before folks take notice.
With that said, there is some good news. I have witnessed an uptake of IVWFMS in recent years. More hospitals seem to be adding these systems to their workflow. While a welcome trend, the increased numbers don’t appear to be secondary to some altruistic good will or common sense, but rather because of Epic. The monolithic EHR vendor has unwillingly changed the landscape of the IVWFMS market, forever. Big pharmacy technology companies refuse to admit it, but the writing is on the wall. When asked what technology a hospital is using in the IV room, I used to hear “nothing” or “DoseEdge” with an occasional “MedKeeper” thrown in. Now, more often than not, I hear “Dispense Prep”.**
Why the shift? No mystery here, the answer is simple: the barrier to entry is low and the integration within the platform is amazing.
For healthcare systems already using Epic, it is as easy as flipping a switch. The implementation requires a bit of legwork, and some minor equipment, but nothing like that required when implementing a third-party system like DoseEdge, BD Cato, etc. I have been involved with both Epic and third party IVWFMS implementations, there is little comparison in time, energy, effort, and cost. Epic Dispense Prep (EDP) wins in all those areas, easily, every single time.
The ease of EDP implementation is tied directly to the modularity and integration of the overall system. It shares databases, labels, user experience, dashboards, and so on. EDP is already part of the EHR, so it requires no additional contracts, no additional maintenance agreements, no third-party vendor helpdesks, no “integration” within the EHR, no crazy implementation schedule and checklists, no weird upgrade schedule or downtime, and so on.
EDP implementation requires far fewer pharmacy resources than other IVWFMS and has the added benefit of being nearly transparent to pharmacy personnel. Most of the build is handled behind the scenes by dedicated IT resources — the ever present Epic Willow Build Team. Pharmacy resources are kept to a minimum, which decreases impact on the department. Contrast this to something like DoseEdge, which requires a significant investment in time and effort from pharmacy personnel. I can attest from personal experience that the overhead for a third party IVWFMS implementation can be hundreds of hours of dedicated pharmacist time. EDP, on the other hand, requires a fraction of that time. This alone makes it an easy choice for pharmacies strapped for resources, which describes nearly all inpatient pharmacies.
None of this means that EDP is the best IVWMS on the market. Not even close. While it offers full integration across the entire enterprise, barcode scanning, image capture, robust tracking, and is seamlessly tied into the billing system — something I care little about but is a top priority for healthcare systems — it falls short in other areas. As I write this, I can think of at least three products off the top of my head that I believe are better than Dispense Prep. They are more flexible, more feature rich, have better hardware, have better software, and so on. Most even eclipse EDP in the quality of the basics, like image capture. But it doesn’t matter if they are never implemented. The best IVWFMS is the one you are using. While Dispense Prep may not be the best, it is better than nothing. Love the one you’re with, you know?
While not an accident per se, I believe Epic won the battle of IV workflow management systems without trying. Several large IDNS have already converted to Epic, giving them an obvious competitive edge in the IV room. As facilities with Epic gravitate toward Dispense Prep for the reasons outlined above, the market will inevitably begin to contract, forcing third party vendors to compete against one another for a smaller piece of the pie. It may take some time – things always do in healthcare – but companies marketing IVWFMS will feel the pressure. I believe some already have. I have personally witnessed facilities that have uninstalled DoseEdge in favor of EDP, and some that have elected to with Epic over an outside vendor. The pressure is on.
To the IVWFMS out there, I wish you good luck. The long game is not in your favor.
===========================
*Robotics has its place in the IV room. Products continue to get better every year. While it may not be for everyone, I can see use cases where robotics would be a viable option.
**EPIC Dispense Prep (EDP) is the IVWFMS module inside the Epic EHR System. It is an incredibly well integrated piece of the overall Epic medication distribution model. Dispense Queue [a dashboard of everything waiting to be prepared] → Dispense Prep [capture all data during compounding] → Dispense Check [Pharmacist Review] → Dispense Tracking [track product from pharmacy to bedside]. While I do not care for Epic, in general, one has to admire the vision and design.
I’ve been writing about the need for pharmacy integration for years. Most of it negative, and deservedly so because it’s been lousy.
With that said, things appear to have changed in recent years. Integration, it seems, has slowly become a thing. Maybe because I’ve been out of general pharmacy practice for so long that it seems decent, or maybe it’s getting better. Hard to tell, honestly.
Pharmacy systems aren’t really talking to each other better than before, per se, but the number of disparate systems seem to have decreased over the years. Once there were many, now there are seeming few. Once, everything was “best-of-breed”, now things are moving to one system to rule them. Case in point, electronic health records. (EHRs).
I always thought pharmacy integration would take place from the inside out, i.e. pharmacy systems would integrate with other systems and drive information sharing across the hospital. Not even close. Instead, pharmacy systems have become more integrated by being consolidated and sucked into the EHR.
The advent of EHRs has done more for system integration in healthcare than just about anything else. I have plenty of negative things to say about EHRs, but it’s clear that they’ve changed the way we practice, forever.
The way I see things, at least now, most healthcare systems have fallen into two large buckets: 1) documentation, clinical, and other; and 2) operational logistics.
Clinical Documentation: Clinical documentation used to take place in “the chart”, among many other places. The chart was nothing more than a binder filled with dividers, separating one bit of information from another. Think of a Trapper Keeper, minus the cool picture on the cover. Paper was everywhere. If you wanted to read something about a patient, like a progress note or radiology report, you had to go to the chart, which wasn’t always easy. They had a way of walking away with physicians and not making their way back to the nursing station.
This all changed when EHRs hit the scene. Everything from demographic data to notes, lab values, medication information, and so on is at your fingertips. If you need information, all you do is log into the EHR and go hunting. Admittedly, it’s not as easy to navigate as a paper chart, but it’s a heck of a lot more data rich and never walks away.
Most of the information coming out of hospital pharmacies these days can be found in EHRs. That includes medication distribution information, pharmacist notes, barcode archives, and so on.
Operational Logistics: Think Amazon warehouse. That is the easiest way I can explain pharmacy logistics. You buy something from a third party, store it in the pharmacy for a period of time, and send it to a patient when it is ordered. Simple, really. We are still not very good at it, but that’s the gist.
For the most part, pharmacy logistics has maintained its distance from the influence of EHRs. Instead, inventory management has been driven largely by a other, non-EHR companies: CareFusion, Omnicell, and to a lesser extent, Swisslog. These companies have grown and expanded over the years, increasing their portfolios to cover more and more areas of the pharmacy.
I have mentioned the “four areas of pharmacy” many times: standard storage, refrigerated storage, controlled substance storage, and the iv room. The first three areas are still dominated by these companies. Carousels, inventory software, refrigerators, various cabinets controlled by remote locks, and automated packagers can be found in most large pharmacies. All of which are offered by the aforementioned companies. There was a time when it was common for any number of these products to be supplied by different vendors. Not so much anymore.
These days, it is all about integrated systems from a single vendor. When given a choice, pharmacies are deciding to purchase from a vendor that can “do it all”. For example, CareFusion offers Pyxis ES ADUs for medication distribution at the point of care; Pyxis Logistics software and hardware for medication distribution from the pharmacy; Pyxis CII safe to manage controlled substances; BD Cato for the IV room; and so on.
With that said, the IV room is in a state of flux. The nature of this area lends itself to both operational logistics and documentation, the latter of which seems to be more important now more than before. It may be the only area of the four where inventory management means less than documentation. I expect this trend to continue. Â
Surprisingly, I really have seen better integration amongst pharmacy systems these days. I fully expect it to improve even more as EHRs expand and eventually creep into operational logistics. At least one EHR vendor has already made a significant impact in the IV room. Eventually, pharmacy will be just another department within the EHR’s web of control. I see both good and bad in such a future, but that’s a blog post for another time.
Full disclosure, anyone reading this should take it with a grain of salt. I used to work for Talyst as a product manager for their acute care product line, and I’ve recently been involved with a Pyxis Logistics implementation. With that said, forward.
In short, yes, BD Pyxis Logistics (“Logistics) is quite good. BD is doing something that pharmacy has needed for a long time, embracing the concept of “the enterprise†with integration across multiple areas in and out of the pharmacy. BD, as a company, has been busy over the past few years piecing together products to create a cohesive strategy. Someone has been paying attention.
Are they there yet? Not yet, but they are on their way. To paraphrase my brother, they’re currently the worst they’re ever going to be, i.e. their products and strategy are only going to get better and mature over time.
You’ve heard me talk about the four areas of pharmacy many times: standard storage, refrigerated storage, controlled substance storage, and the iv room.
Basic storage are those basic shelving units that most people think of when they walk into a pharmacy. It’s where you’ll find unit-dose and bulk room-temperature items. Logistics is squarely focused on this area of the pharmacy. It works well and, at least in my opinion, does a good job of addressing inventory across multiple pharmacies. Throw in that Logistics is web-based, and it’s compelling.
Refrigerated storage is, well, where you put things when you want to keep them cold. Same as basic storage, only refrigerated. BD doesn’t offer anything specific for this area, but Logistics handles refrigerated items just fine. It basically treats refrigerators the same way it treats static shelving and carousels. It’s just another storage area.
Cleanroom/IV Room is where you’ll find all the supplies for compounding sterile medications. The IV room has been getting a lot of attention lately, but that has nothing to do with inventory management. Most pharmacies treat the IV room as a black hole for inventory, i.e. they lose visibility of their inventory when it crosses the threshold into the land of sterility., BD has had a product called Cato for many years. It’s now called BD Pyxis IV Prep and I’ve always been a fan. Pyxis IV isn’t fully integrated with Logistics, but they’re working on it.
Controlled substance storage is where you’ll find all your opioids, benzodiazepines, and so on. Anything the DEA, Board of Pharmacy, and any other regulatory agency considers a diversion risk. I have a love-hate relationship with controlled substance management. This area is long overdue for improvement. With that said, I’m happy to report that BD is making inroads. The latest version of their CII safe software is integrated with Logistics, meaning no more disparate systems for controlled and non-controlled meds.
What I like about Pyxis Logistics
Multiple pieces of the pharmacy puzzle. When looking at the BD Pyxis lineup, the four areas of pharmacy are closer than ever.
Integration that is getting better and better all the time. BD not only has the pharmacy covered — Logistics, CII Safe, IV prep — but think about their dominance in the automated dispensing unit (ADU) market. Integration is hard, but getting ADUs and pharmacy inventory seamlessly talking to one another is something I’ve been pining after for a long time. Â
Handhelds. BD offers a handheld for Logistics. I haven’t had one in my hands but the device and functionality look good, shortening the inventory gaps even more. Talyst had a handheld device for AutoPharm years ago. Wonder what became of it?
Good folks to work with. I have nothing but good things to say about the people from BD that I’ve worked with. They want to do a good job.
Improvements are rapid and obvious. That’s the thing about most companies, they want to improve their products and keep customers happy. Improved products and happy customers equal increased adoption, which in turn leads to more sales, which leads to more money, and so on down the rabbit hole.
What I don’t like about Pyxis Logistics
Reports and analytics appear weak. The system offers many canned reports and access to the company’s Knowledge Portal, but overall, it feels like they’re behind in this area. From what I’ve seen, it’s just not there. When compared to something like the analytics software from Swisslog — still don’t know the name of the product…. Pharmacy Analytics? I mentioned it here — it feels miles behind. What’s worse is that what I saw at ASHP Midyear back in December doesn’t make me feel any better about it.
Piecemeal products. It’s obvious what BD is doing. However, buying products and folding them into your portfolio can make things feel like they’re bolted on instead of feeling like they’re an integral part. It’s only going to get better, but one has to be willing to ride through the rough patches to get to the smooth road.
Lack of product maturity. “Pyxis”, the ADUs, is a very mature product that’s used in thousands of facilities. Logistics and IV Prep, not so much, and it feels like it.
Overall, it seems as though BD is heading in the right direction. It will be interesting to see where the company ultimately goes with their strategy.
Several years ago,
shortly after I was let go from Talyst, I found myself with some free time on
my hands. I started writing a book. The book was titled ‘Making the right
choice: Helping pharmacies make smart decisions about automation and technology’.
Like many books I’ve started, it remains unfinished. I don’t think I’ve touched
it since 2016. At least that’s the date I have listed as the last time I edited
it. However, I recently had reason to go back and review some things I included
in the book. Kind of a retrospective review of advice to myself.
Specifically, I was interested in my thoughts on putting together a project team and managing a project. And there, in Chapter 8: First things first, I found what I was looking for. Some of the information is outdated, specifically the final page called Cautionary Tale**, but overall the information still rings true.
Here it is,
Chapter 8 in it’s draft form. Maybe one day I’ll get around to finishing the
book. One never can tell.
Chapter 8: First things first
“You can do anything…but before you can do anything, you have to do something.†— Clifford Cohen
You can’t get
to the end of a project if you never start, and getting started can often seem
like the most difficult part of any project. I can’t pinpoint why it’s so hard
to get started, but it is. Perhaps it’s fear of the unknown, or unwillingness
to move away from comfort zones. Or maybe it’s because we don’t want to do the
work. Who knows? The only thing I know for sure is that once the ball gets
rolling, no matter how slowly, it always seems to roll forward. The key is to
stop putting it off and get started.
With that
said, it’s important that one is truly ready to move forward. Understanding the
reason(s) for doing something is key. Seems simple, but it might surprise you
to learn how often people do things without understanding why. Begin the process
with eyes wide open. Never do anything simply for the sake of doing something.
One must be
able to justify all projects, regardless of their purpose. Simply put, the
project must worthwhile, viable and affordable, bring a reasonable return on
investment (ROI), and be within acceptable tolerances and risks.
Ask yourself these three questions:
What do I hope to accomplish?
Does the technology make sense?
Does the technology fit my operations
If you’ve
answered the above questions to everyone’s satisfaction, it’s time to get
busy.
Below are the
things that I think are important to ensuring a successful technology implementation
in a pharmacy. While it may seem like a lot of work, the end result will be
worth the time and energy.
Gauge user
beliefs and feeling. Is
it going to be an uphill battle? Are the pharmacists and technicians open to
the idea of implementing new technology? Is the pharmacy morale where it should
be? Does your department fear change? The success of your implementation will
rely heavily on how well you and your department are prepared. The
implementation of new technology can often pose a threat of reduced control
over one’s work. This can create pushback from the staff. Helping them
understand what it is you hope to accomplish, how it will help them, and
offering opportunities for staff to become involved and have a vested interest
in the project can go a long way to ensuring a successful implementation.
Get
support / buy-in for the project.
The need for support for any project is a must, and this is especially true for
pharmacy projects. Success depends on support from the top of the organization
to the bottom. Lack of support will result in a failure to launch. If and when
possible, it is best to start with an executive sponsor, or someone from the
Hospital Board of Directors, if you have one. This person, or persons, will be
your champion during high-level meetings within the organization.
Once you have
executive level support, it’s time to consider support from other areas. If the
project will impact nurses, find a nurse. If a physician, find a physician.
And, so on. You don’t want to launch a project that will impact a group of
people without getting their support. Trust me, it’s not a good idea. Call it
politics if you must, but peer-to-peer communication works wonders. Having
support from a variety of areas and disciplines will improve communication and
go a long way in generating support for a project.
Create a
buzz. Create some
excitement. Don’t act like the project is required, but rather a choice that’s
going to make things better.
Give
everyone fair warning of what you plan to do. People fear change. Give them plenty of time to get
used to the idea. This will go a long way in gaining support for a project.
Being aware of what’s coming is always preferable to being surprised by what
has already been done.
Involvement
and participation. When
individuals believe that a project is relevant, they are much more likely to have
a positive attitude toward it. And the best way to get individuals to believe
is to get them involved. Allow them to participate in all phases of the
project. “Increasing user participation … enhances post-development user
involvement and attitude†(Vaughan PJ. System implementation success factors;
it’s not just the technology. Internal Report of Information Technology
Services. University of Colorado at Boulder. 2000), which is what you
want.
Involve as
many as you can as often as often as you can. When people are involved, it
gives them a sense of ownership and a vested interest in making a project
successful. It also helps deal with negative vibes from others. Include
multiple disciplines, depending on the technology and departments affected.
It is also
important that all participants be volunteers. Mandated participation has been
shown to be ineffective and potentially detrimental to the success of this type
of project. (Hunton, James E., and Jesse
D. Beeler. “Effects of User Participation In Systems Development: A
Longitudinal Field Experiment”. MIS Quarterly 21.4 (1997): 359.
Web. 8 Apr. 2016.)
Champions.
Champions are those people
that go above and beyond the general participant. Champions believe in the project
and the benefits it will provide. They can often have a contagious zeal about
the project, and are sometimes referred to as “evangelistsâ€, or in extreme
cases “zealotsâ€. Whatever you call them, when it comes to implementing new
technology in the pharmacy, Champions can be your best source of support. They
can be useful in putting a spotlight on the project in a positive way and
swaying the negative feelings of others.
Finding
Champions shouldn’t be too difficult. They’re usually early adopters and will
take the initiative to learn more about a project without being asked.
Develop rules for participation. This is really quite simple. It is important that the rules for participation be laid out well in advance, and that each member of the team sign off on them. There should be no surprises for what’s expected from participants once the project is underway. The following rules are examples:
Be willing and able to engage in the
project
Be willing to be positive about the
project
Be willing to work with others to
advance the project toward accomplishing the goal
Be willing to commit to attending
meetings
Be willing to commit to handling extra
work, even if it means staying late or doing some reading at home in the
evenings or on weekends. I understand that no one wants to put in a bunch of
unpaid overtime on these projects. However, on occasion, a little extra work may
need to be done to keep things moving forward. One should enter into
participation with the understanding that this could happen.
Be willing be engage in every aspect
of the project, not only the items that are assigned. It is vitally important
that each participant have at least a basic understanding of the overall scope
of the project and what each member of the team is assigned. Things happen.
People get sick, quit their jobs, move to another state, and so on. Unforeseen
events should not completely derail the project timeline or goals.
Find
naysayers and sway them over to your side. Every project has its opposition. As the saying goes,
you can’t please everyone all the time. Unfortunately, naysayers tend to have vocal
personalities. They’re not afraid to say what’s on their mind. These two things
– being negative and outspoken – tend to go hand-in-hand. The downside to
naysayers is that outwardly negative comments about a project have a way of
spreading like wildfire. They can be caustic, seeping into the minds of even
the staunchest supporter. And once there, negative thoughts can grow like a
cancer. With that said, naysayers and their negative comments have their place.
Because they’re not afraid to speak up, they can sometimes point out things
that others fail to see, helping avoid potential pitfalls. The trick is to use
the information to your advantage. Allow naysayers to offer up their thoughts
in a controlled environment where their comments can be contained. Give them
space to vent. Listen to what they have to say. Use what you can and toss the
rest. Showing naysayers that you’re willing to listen and take their concerns
seriously can go a long way. In rare cases, you might even make a convert out
of one, which would be a huge victory for the project. However, never try to
force change on a naysayer. Forcing change, or mandating them to join your side,
rarely works. It’s like dealing with a donkey, the harder you pull, the harder
they resist.
Build your team. According to Harvard Business Review’s (HBR’s) 10 Must Reads On Emotional Intelligence[(HBR’s 10 Must Reads On Emotional Intelligence. Print.), a source of great team success lies with teams that can achieve high levels of participation, cooperation, and collaboration among members. Sounds logical, but oh so difficult to do.
Note: HBR’s 10 Must Reads On Emotional Intelligence is a great collection of previously written articles pulled together into a single book. Each article is informative and interesting in its own right. However, when combined, they create a great collection that any person involved in a project should read. I highly recommend it. It’s a short book and an easy read.
Team
members must be chosen carefully and meet three basic conditions:
Mutual
trust of one another
Have
a sense of group identity: a feeling that they belong and the project is
worthwhile
Have
a sense of group efficiency: belief that the team can perform well and that the
group is better than the individual members.
Collectively,
HBR refers to this as the groups “emotional intelligence†(EI). While intelligence
and experience among group members is important, EI may be more important
still. Keep that in mind when you begin building your project team.
Chose
a project leader. Ah,
the leader. The captain. Thy person in charge. It’s a burden that many well
qualified individuals shy away from. Someone has to be in charge. Someone has
to be given authority over the group and be willing to make the tough decisions
and hold people accountable.
Not
everyone is cut out to be a leader. Everyone reading this has worked for both
great and terrible leaders. While I cannot tell you exactly how to identify a
great leader, I know one when I see one.
According to HBR’s10 Must
Reads On Emotional Intelligence
what distinguishes good leaders from great ones is their EI. For individuals,
EI is “a group of five skills that enable the best leaders to maximize their
own and their followers’ performanceâ€.
The
EI skills are:
Empathy
Motivation
Self-regulation:
controlling negative impulses [side note: this is really hard to do, especially
during high-stress times]
Self-awareness:
knowing strengths and weaknesses
Social
skill: being able to build a rapport with others to get desired results {side
note: especially tough if you’re a natural introvert]
Find
yourself a project manager. As
ridiculous as this may sound, the project manager is an often overlooked
position when discussing project teams. Let me go on record now as saying that
a good project manager is absolutely vital to the success of any project, and
could arguably be considered the linchpin to the success of the entire project.
It
is the job of the project manager to manage all aspects of the project,
including the scope, timeline, cost, quality, and people. They apply their
knowledge, skills, tools, and techniques to help projects be successful.
“The
role of the project manager is that of an enabler. Her job is to help the team
get the work completed, to “run interference†for them, to get scare resources
that they need, and to buffer them from outside forces that would disrupt the work.â€
(Lewis, James P. Fundamentals Of Project Management. New York: American
Management Association, 2007. Print.)
Things
to consider when selecting a project manager:
The
person must have leadership qualities, have good self-management and time
management skills, and be a taskmaster.
The
project manager cannot serve two masters. Individuals
that serve as a project manager must not be required to do any of the actual
work in the project. According to James Lewis, “as team sizes increase,
it becomes impossible to work and manage both [the work and the team], because
you are constantly being pulled away from the work by the needs of your team
membersâ€. Having project managers attempt to manage the project and perform
work in the project is a recipe for disaster.
The
person must have a proven track record. We all know people that can’t manage
the paper piles in their office much less a multi-faceted project requiring
meticulous attention to detail.
I
encourage everyone involved in a large project to read a book or two on project
management. Being a project manager is not as easy as it sounds and should be
given the respect it deserves.
**Cautionary Tale. Since drafting this section of
the book, I have been involved in another amazing project. One that had me
working with large teams to remodel or construct new pharmacy cleanrooms for
several hospitals. The project spanned well over a year and was simply
incredible.
There was an interesting thread in one of the ASHP practice forums recently. Someone asked whether or not pharmacists were “ready for the future that the opportunities these disruptive technologies offerâ€. This in reference to technologies that they saw in the exhibit hall at ASHP Midyear.
The simple answer is no. Pharmacists are barely ready for technology that’s 20 years old, much less anything that is disruptive. In support of my quick answer, I give you a brief conversation I had with one of the most progressive pharmacy operations people I’ve ever known (paraphrased, of course):
Me: “See anything cool in the exhibit hall?”
Them: “Yeah, a change in software that will allow me to capture more 340B costs in the OR.”
Me: “Really? What about Kiro, IntelliGuard, and PharmID?”
Them: “That stuff? I don’t care about that stuff. It’s meaningless to me because it doesn’t help me. Not to mention that my organization will never go for it.”
The ASHP forum thread produced some interesting responses. One pharmacist pointed out that healthcare disruption will come from outside of healthcare. I agree with that opinion 100%. However, someone responded that they didn’t think this was “… a foregone conclusion†because they think that “…in the short to medium term, in order to actually make meaningful improvements in outcomes, healthcare needs to be disrupted from withinâ€. I almost snorted coffee out of my nose when I read that. It was that funny.
I’ve been a pharmacist for more that 20 years. In that time, pharmacy hasn’t disrupted anything. Nothing. Nada. Pharmacy departments are so busy keeping up with regulatory requirements and chasing elusive “clinical activities” that they don’t have time to innovate and disrupt.
I went back through some of my posts from the past few years. Here’s what I found:
03/02/15: 5 years later, my thoughts on pharmacy practice — “Pharmacy is the same as it was when I left. It’s the same chaotic, messy thing that it’s always been…. Five years out of the game and I don’t feel like I’ve missed much.”
06/04/15: Pharmacy – entrenched in outdated dogma — “…you should be using the most complete solution possible in the i.v. room, and you need to get over the idea that a PharmD is required for a “final checkâ€.”
09/20/15: Will healthcare disruption come easy and fast? — “There are many things being developed to improve healthcare, but the innovation is coming from outside sources. People are literally leaving healthcare to innovate things for healthcare.”
11/10/16: Someone please disrupt controlled substance storage technologies — “Management of controlled substances inside acute care pharmacies is a mess… Based on my observations, the technology is outdated, difficult to use, and has failed to improve the process in any appreciable way. It remains unclear to me what advantage these systems offer.”
09/21/17: It’s time to disrupt pharmacist order verification — “It’s an antiquated process that’s long overdue for an overhaul. The time has come for healthcare systems to make better use of their personnel.”
And that’s just flipping through my posts from the past few years. I can’t imagine what I’d find if I went all the way back to the birth of this weblog in 2009.
I used to think about disrupting healthcare all the time. I recorded my ideas in notebooks and spent years pitching my ideas to companies in the hopes of building a new and exciting pharmacy practice. But it went nowhere, and became nothing more than an exercise in futility.(1)
Is there a healthcare company out there that will disrupt pharmacy? Not likely. As a really smart lady once told me, no one wants to be in this space because it’s hard and you can’t make any money. What about companies from the outside? Also not likely for the same reason.
If it sounds like I’m bitter about all this, it’s because I am. Pharmacy practice could be so much more if we’d just crawl out of our holes and do something different from time to time.
Here’s the bottom line, pharmacy needs to be disrupted — desperately. However, it’s not going to happen. The best we can hope for are iteratvie changes, at best.
=============== (1) I’ve actually had a few ideas turn into real products. Nothing earth shattering, but cool nonetheless.
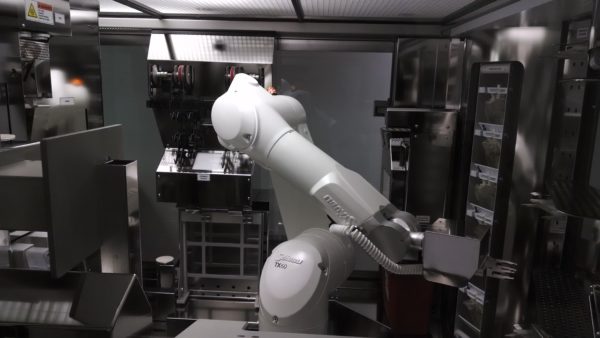
I love pharmacy IV room workflow and technology, but I don’t get to talk about it much anymore. Most of my conversations these days are focused on IV room regulation, i.e. compliance with USP <797>/<800> and Board of Pharmacy rules. So you can imagine my surprise when two people approached me on two completely different occasions at two unrelated events asking my thoughts on IV room technology. Awesome! Then they asked me what I thought about using robots in the IV room. Bummer. Of all IV room technologies, robotics is my least favorite.
Image owned by Jerry Fahrni, Pharm.D. Taken February 12, 2014.
Ten years ago, I was optimistic about IV room robots. Today, not so much. If I could sum up my opinion in one sentence, it would be that highly-automated robotic systems for sterile compounding are not ready for prime time. Note that I said highly-automated and not fully-automated. Even though robots replace human hands for the actual compounding process, they are dependent on human hands for moving products in and out of the robot before, during, and after the compounding process. When considering IV robotics, one should always think about:
Patient safety – Can robots reduce CSP errors? Certainly, but so can most any IV room technology that utilizes bar-code scanning, gravimetrics, imaging, etc. Often times people will tout robotic systems for consistently compounding drugs within 5% of the prescribed dose. It’s not really a big deal. Doses slightly outside the 5% range are not clinically significant, and getting it within that range is not important enough by itself to warrant the investment in a robotic system. Given proper guidance and a system for compounding, particularly an IV workflow management system, humans can easily be as accurate.
Worker protection from hazardous drugs (HDs) – There is no question that IV robots have the potential to reduce worker exposure to HDs during the compounding process. Then again, new USP <800> guidelines do the same. Ever heard of a CSTD?
Workflow efficiency – Not sure a robot brings you increased efficiency unless you’re talking about single batch high-volume IV production. I sat for hours watching IV robots doing their thing in pharmacy cleanrooms across the country. I don’t think I ever thought to myself, “dude, that thing sure makes things easier/betterâ€.
Cost reduction from moving outsourced CSPs back in house, i.e. no longer having to purchase CSPs from a third party – Not specific to robots. Perhaps for single batch high-volume IV production, but doubtful.
Reduced waste from discontinued orders falling off work queues before they are filled – Sure, a robot can help with this, but the same is true for almost any IV workflow management system.
Comprehensive documentation for regulatory compliance – These systems certainly collect lots of data but how easy is it to use? Just because the system collects info doesn’t mean you can get it out when you need it. I’ve seen things. Just sayin’.
Return on investment (ROI) – What do these systems give back? There are few pharmacies where IV room robots will result in a positive ROI. I’ve seen pharmacies try. While their arguments may sound good on paper, in practice they are as thin as the paper they are written on. The only time these systems yield a real ROI, in my opinion, is when they are used to repetitively compound the same few items over and over again – in other words, batch compounding for high-volume items. All of the systems have roughly the same throughput, which is much lower than that of a highly skilled technician. IntelliFill i.v. is the fastest of all the robots I’ve seen, but it is limited in scope to syringes.
Formulary limitations – One of the major limitations of IV robots is the number of formulary items they can handle. During visits to facilities using IV robots — San Francisco, CA; Asheville, NC; Baltimore, MD; Madera, CA; and so on — I saw very few medication “line items†assigned to the robot. The largest number I witnessed was somewhere around 10, and the smallest number was two. Two! Someone had a million-dollar robot making CSPs out of two drugs. Hospital formularies are large and diverse. They include all kinds of IV products: piggybacks, large-volume parenterals, syringes, and so on. Not to mention that formularies change all the time. The inability of these systems to manage a large number of different CSPs at one time is definitely a limitation.
Maintenance – What does it cost to maintain these bad boys? They don’t operate on a zero cost. They also don’t maintain themselves. Operational resources required for things like robot maintenance, formulary maintenance, product changes, and so on are important considerations to keep in mind when purchasing a robot. Who is serving who…. or is that who is serving whom? I can never get that right. Anyway, the time, energy, and effort required to keep an IV robot at peak operational efficiency simple isn’t worth it. At least not in my opinion. In a nutshell, I’m just not a fan of the current crop of IV robots. Does that mean that there is no future for robots in sterile compounding? On the contrary, I think we must move toward a future where all CSPs are made by robots. It’s the only thing that makes sense. Unfortunately, that future is still far off. I’ve had the opportunity to peak behind the curtains at a few robots currently under development. There are some great products coming down the pike, but we are going to have to wait a while. Apparently, building robots with creative new features is hard.
A large portion of the most recent issue of the ISMP Medication Safety Alert is dedicated to IV workflow management systems (IVWFM) and errors caused by workarounds. There are a few head-scratchers in the list to be sure. There are even some that had me speculating their authenticity, i.e. too wacky to believe.
“Data submitted to the ISMP National Medication Errors Reporting Program (ISMP MERP) have repeatedly shown that manual verification of intravenous (IV) admixture ingredients by pharmacy personnel who prepare solutions and pharmacists who inspect the final products is not particularly effective in detecting and correcting errors.” You can take this to the bank! Rule #1: people are people. They make mistakes and do crazy things sometimes. Rule #2: no amount of technology will eliminate rule #1.
“However, as with any new technology that introduces an element of change, we want you to know about the workarounds and errors we have learned about with WFMS and why they may be happening so you can be as prepared as possible to address the when you assess or implement this technology. Some of these workarounds or errors are common to many other forms of healthcare technology.”
This is no doubt true as I’ve witnessed workarounds with pharmacy technology on many occasions.The sad truth of the matter is that no amount of technology will prevent people from finding workarounds. Just like no amount of manual processes and double checking will prevent workarounds. Unfortunately, these workarounds can lead to mistakes, which is what we are ultimately trying to prevent.
Typically, it is a combination of well-defined processes with appropriate technology that creates the safest environment. It’s also the best way to prevent workarounds. That and opening a can of whoop ass on people that don’t follow the rules; figuratively speaking, of course.
Here are some of the potential workarounds and errors identified by ISMP, many of which are similar to those seen with bar-code medication administration (BCMA):
Inability to scan the barcode — This is a common problem with any bar-code scanning process, i.e. BCMA, etc. Barcodes are far from perfect and will never be 100% scannable.
Reluctance to scan the barcode — Human nature. Go figure.
Scanning just one vial — i.e. scanning a “representative vial” when using more than one vial during CSP prep. Happens all the time.
Using a decoy for scanning or image capture — the old barcode-in-the-pocket scam.
Using the syringe pull-back method — hard to imagine that this is still going on in pharmacies across the country. It should be banned. Any facility caught using the syringe pull-back method should be fined heavily and mocked openly for their laziness.
Blurry or missing digital images — I’ve experienced this personally. Here are some images from one popular IVWFM system that were given to me. Can you tell, without any doubt, what the volumes are in these syringes? [If anyone has any sample images, I would love to see them]
Lapses in technique. “Use of WFMS touch screens can lead to touch contamination, especially when handling hazardous drugs. This and other lapses in hazardous drug handling and aseptic technique are not easily captured by the WFMS and may go unnoticed.” — No doubt a problem. Regardless of what technology you add to your process, proper technique in the hood is a must.
Interference with the scale. “ISMP has received a report about a WFMS with gravimetric technology for which the scale would not work in a laminar airflow workbench/biological safety cabinet due to vibration. Every time the pharmacy technician needed to weigh a product, he or she had to turn off the hood [what the heck!].” — not all gravimetric solutions are equal. There are at least two IVWFM systems on the market that do a great job with their gravimetrics. There is at least one that doesn’t. Any facility considering this technology should make sure to do their homework.
This came through one of my Google Alerts this morning.
Life Pulse Health Magazine: “Pearson Medical Technologies’ [PMT] … m:Print Version 3.9.1 has been updated to use Microsoft SQL Server 2012/2014 for more efficiency and advanced performance. Each packaging run can now automatically generate a unique lot number. Most importantly, Pearson Medical has added a bar code constructing module which allows users to add more than one drug information into a bar code… in addition to the release of a new version of m:Print , we have selected Medi-Span to provide the drug database for use within m:Print.â€
m:Print is a great stand-alone option for pharmacies looking to print bar code labels for vials, ampules, syringes, IV bags, etc. The system is well liked by many. In fact, PMT has OEM’d m:Print for other companies as their bar code printing solution. So if you have an inventory management system from another company and m:Print looks familiar, that’s probably because it’s the same software, minus some minor UI tweaks.
I personally like m:Print, mostly due to its flexibility. It offers the ability to use virtually any printer or label type. You can customize labels just about any way you see fit, including the use of 2D and/or linear bar codes.
I had the opportunity to get a sneak peak of m:Print version 3.9.1 prior to its release. Overall, there are some nice improvements. Chances are, if you liked the system before, you’re probably going to like it even better now.
————–
Disclaimer: as a consultant, I’ve done work for PMT and with companies that have partnered with PMT.
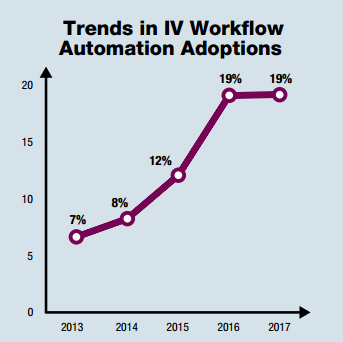
Pharmacy Purchasing & Products (PP&P) puts out a survey each year called The State of Pharmacy Automation (SOPA). The 2017 PP&P SOPA is out and available for your reading pleasure.
The PP&P SOPA survey covers many automation, technology, and practice trends. One item that I look at each year with great interest is the reported IV workflow management system (IVWFMS) adoption rate. I’ve written about IVWFMS many times. I even went as far as to do a podcast dedicated to them back in 2015.*
While reviewing the 2017 SOPA numbers, I was surprised to see that this year’s survey shows no gain in adoption of IVWMS over last year. They appear to be stalled at approximately 19%, same as last year (see graph from PP&P 2017 SOPA below).
While informative, it’s important to take these survey results with a grain of salt. Response rates are incredibly low, for one thing. Results can also be skewed based on participants, i.e. it may not be the same pharmacies responding year over year. This makes it difficult to draw direct comparisons from one year to the next.Â
Regardless, I was still surprised to see the flattened curve. I expected to see a sharp uptake. Most facilities I go into these days are using, or in the process of implementing, an IVWFMS of some kind. It’s becoming less common to find a facility not using one of these systems, especially in larger facilities where they seem to be slowly becoming best practice. Â
One other item worth mentioning is my belief that last year’s survey overestimated the number of facilities using IVWFMS. So if last year was really 12-15%, perhaps this year’s result is an improvement. That’s purely speculation on my part. I have nothing concrete to back it up other than my sense of the market. Through no fault of PP&P, I feel like these surveys are a poor representation of what’s really going on in the real world.
Other takeaways from this year’s survey:
Larger hospitals are adopting IVWFMS faster than smaller hospitals. No surprise here. If you’re a hospital with more than 400 beds and you haven’t implemented one of these systems, you’re wrong and should be embarrassed by your lack of action. “Ninety-nine percent of the failures come from people who have the habit of making excuses.” ~ George Washington Carver. Simple as that.
DoseEdge by Baxter is the #1 system in use. Again, no surprise. This corresponds to what I see in the wild. Baxter has been in the game for a while. DoseEdge is definitely the first system that comes to mind when talking about IV room technology. Pharmacy Keeper by MedKeeper at #2 is a bit of a surprise. I have yet to go into a pharmacy that is using it. It’s a less functional system than say DoseEdge or BD Cato, but it’s also less expensive and easier to install, implement, and maintain. I personally believe pharmacies should be looking at systems with proven gravimetrics, but that’s just me. Pick your own poison.
DoseEdge by Baxter is the #1 system under consideration for new implementations. BD Cato comes in at #2 by a small margin. DoseEdge at #1 surprises me a bit. Most facilities I go into these days have BD Cato at the top of their list of possibles, and for good reason. BD Cato has a lot to offer, especially now that they are part of CareFusion. Perhaps the survey is a bit behind what I’m seeing out in the wild. Impossible to say.
That’s it. I’m not sure that the raw numbers presented in the survey are helpful, but the information in the SOPA survey goes way beyond the numbers. For instance, the SOPA may introduce pharmacies to vendors and technologies that they’ve never heard of before. I encourage everyone to read through the PP&P 2017 SOPA. Who knows, you might find something new and exciting in there. I’ve been doing this for many years, but I still get surprised from time to time.Â
I can’t explain the SOPA survey results, but overall it feels to me that adoption of IVWFMS is still on the rise.
—–
*Looking back through some of my old posts — and the podcast — it’s amazing how little this landscape has changed.
I’m a little slow getting to my thoughts on this deal.
A couple of weeks ago it was announced that Talyst had been acquired by Swisslog Healthcare. I’ve known about this acquisition for a while so I wasn’t surprised when it finally went through. Since the announcement, I’ve reached out to some friends and colleagues on both sides of the fence to get their thoughts and opinions on what’s in store for the future.
My contacts at Talyst have been quite helpful and informative. Swisslog, not so much. In fact, they’ve provided me with no additional information or insight. All they’ve done is sic their marketing department on me, who in turn sent me a bunch of marketing hype that I can find online. Useless. I hope this isn’t a primer on what we can expect from the “new Talyst†moving forward. That would be unfortunate. I suppose this is the difference between a small company and a large company. I’ve always had trouble getting good information from large companies. There are simply too many layers to get through. With small companies, I can often go directly to the CEO. In large companies, I’m met by an army of people designed to keep people like me away from the CEO.
Trying to figure out what Swisslog wants with Talyst has given me much to think about. Talyst is a market leader in certain acute care areas of pharmacy, such as carousels and inventory management software. They aren’t particularly creative or innovative, but rather steady. Talyst knows carousels but that market has kind of run its course unless you’re building a new pharmacy. The high-speed packaging market in acute care pharmacies is basically dead. The company doesn’t offer a competitive controlled-substance management system. They have a solid refrigeration strategy, but it’s not as innovative as something like Evolve. Talyst doesn’t do anything with RFID technology nor do they have a mobile strategy. Their software has good functionality but is antiquated in many ways. So what it is that Swisslog wants? Customer base? Name recognition?
Swisslog doesn’t have much of a footprint in acute care pharmacies except for their tube system, which is basically everywhere. However, Swisslog is creative and innovative. They have some robotic systems like BoxPicker, PillPick, and RoboCourier. They make use of RFID technologies. They have pretty decent integration within their systems and they’re really good at logistics. Honestly, I don’t know as much about Swisslog as I do Talyst.Â
In general, I like products from both companies. However, it’s hard for me to imagine where Talyst products will fit into the Swisslog scheme. The items I think Swisslog needs from Talyst will likely be the most difficult to use, i.e. think square peg and round hole. I suppose the existing Talyst customer base is something that Swisslog can take advantage of. Customers using Talyst products could benefit from Swisslog products and better integration across the two platforms. That goes vice versa as well.
Only time will tell, but I’m betting that we won’t see anything significant from this deal for quite some time.