A large portion of the most recent issue of the ISMP Medication Safety Alert is dedicated to IV workflow management systems (IVWFM) and errors caused by workarounds. There are a few head-scratchers in the list to be sure. There are even some that had me speculating their authenticity, i.e. too wacky to believe.
“Data submitted to the ISMP National Medication Errors Reporting Program (ISMP MERP) have repeatedly shown that manual verification of intravenous (IV) admixture ingredients by pharmacy personnel who prepare solutions and pharmacists who inspect the final products is not particularly effective in detecting and correcting errors.” You can take this to the bank! Rule #1: people are people. They make mistakes and do crazy things sometimes. Rule #2: no amount of technology will eliminate rule #1.
“However, as with any new technology that introduces an element of change, we want you to know about the workarounds and errors we have learned about with WFMS and why they may be happening so you can be as prepared as possible to address the when you assess or implement this technology. Some of these workarounds or errors are common to many other forms of healthcare technology.”
This is no doubt true as I’ve witnessed workarounds with pharmacy technology on many occasions.The sad truth of the matter is that no amount of technology will prevent people from finding workarounds. Just like no amount of manual processes and double checking will prevent workarounds. Unfortunately, these workarounds can lead to mistakes, which is what we are ultimately trying to prevent.
Typically, it is a combination of well-defined processes with appropriate technology that creates the safest environment. It’s also the best way to prevent workarounds. That and opening a can of whoop ass on people that don’t follow the rules; figuratively speaking, of course.
Here are some of the potential workarounds and errors identified by ISMP, many of which are similar to those seen with bar-code medication administration (BCMA):
Inability to scan the barcode — This is a common problem with any bar-code scanning process, i.e. BCMA, etc. Barcodes are far from perfect and will never be 100% scannable.
Reluctance to scan the barcode — Human nature. Go figure.
Scanning just one vial — i.e. scanning a “representative vial” when using more than one vial during CSP prep. Happens all the time.
Using a decoy for scanning or image capture — the old barcode-in-the-pocket scam.
Using the syringe pull-back method — hard to imagine that this is still going on in pharmacies across the country. It should be banned. Any facility caught using the syringe pull-back method should be fined heavily and mocked openly for their laziness.
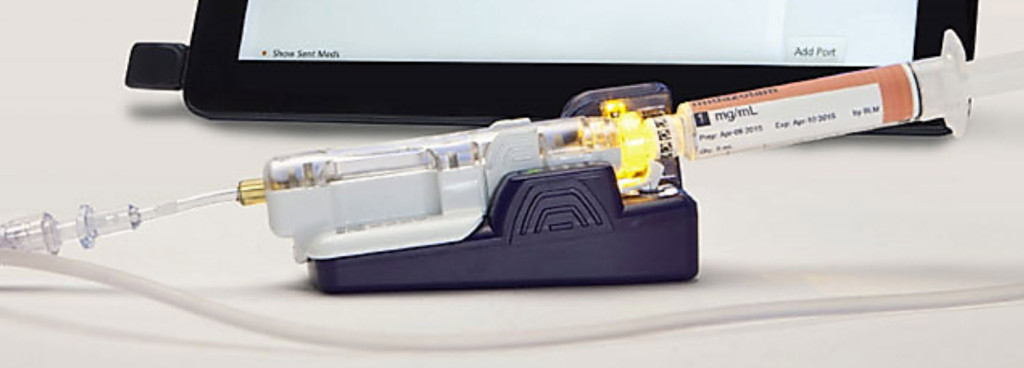
Blurry or missing digital images — I’ve experienced this personally. Here are some images from one popular IVWFM system that were given to me. Can you tell, without any doubt, what the volumes are in these syringes? [If anyone has any sample images, I would love to see them]



Lapses in technique. “Use of WFMS touch screens can lead to touch contamination, especially when handling hazardous drugs. This and other lapses in hazardous drug handling and aseptic technique are not easily captured by the WFMS and may go unnoticed.” — No doubt a problem. Regardless of what technology you add to your process, proper technique in the hood is a must.
Interference with the scale. “ISMP has received a report about a WFMS with gravimetric technology for which the scale would not work in a laminar airflow workbench/biological safety cabinet due to vibration. Every time the pharmacy technician needed to weigh a product, he or she had to turn off the hood [what the heck!].” — not all gravimetric solutions are equal. There are at least two IVWFM systems on the market that do a great job with their gravimetrics. There is at least one that doesn’t. Any facility considering this technology should make sure to do their homework.