I spent a short time observing iv preparation in two separate, distinctly different pharmacy environments in the weeks leading up to the new year.
One was a traditional iv room in a large acute care pharmacy with multiple pharmacy technicians and pharmacists putting out hundreds of compounded sterile preparations (CSPs) per day. The second was a segregated compounding area in a satellite pharmacy with one pharmacy technician and one pharmacist using a glove box to prepare STAT and first dose CSPs to critical care areas.
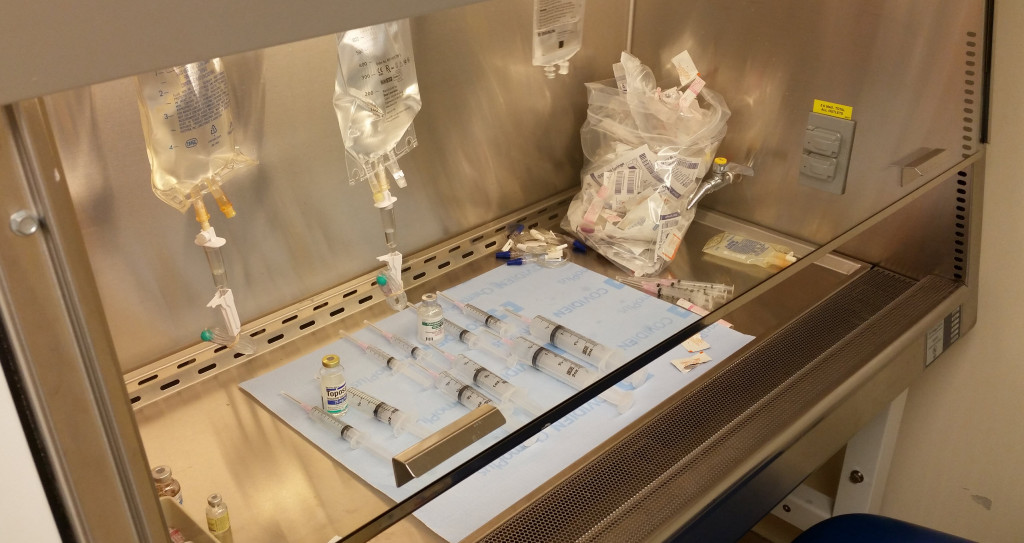
Neither area utilized technology for CSP preparation, instead opting for the good ole fashioned syringe pull-back method (1). In the case of the traditional iv room, I observed instances of up to twenty different CSPs with empty vials and syringes laid out awaiting pharmacist verification. In the segregated compounding area with glove box, CSPs were typically prepared one at a time or in small batches.
During my short time observing CSP preparation in the two areas I witnessed errors that would have easily been caught with the use of readily available technology. Â Here are two examples:
Wrong drug selection – This may be the most common error seen in iv rooms. In this particular case, the technician used a vial of potassium phosphate (KPhos) for a CSP that called for sodium phosphate (NaPhos). The use of bar code scanning for verification during the compounding process would have prevented this error.
Calculation error resulting in an incorrect dilution – A patient-specific order called for 20 mg of hydrocortisone in a total volume of 2 mL to be placed in a syringe for iv administration. The technician started by first making a stock hydrocortisone syringe from which to draw the dose. This is a common practice. The resulting stock syringe should have contained 100 mg of hydrocortisone in 10 mL of solution, i.e. final concentration of 10 mg/mL. Instead, the technician calculated the final volume as 25 mL, resulting in a final concentration of 4 mg/mL in the stock syringe. So when the patient-specific dose of 2 mL was drawn into the syringe the final dose was only 8 mg. The pharmacist almost let it go, but something made him take a second look. It was only when he asked the technician to explain the process that the error was discovered. The use of bar code scanning for verification during the compounding process would not have prevented this error. But, the use of step-by-step instructions with intermediary step checks during the stock syringe prep, or the use of gravimetrics, would have.
The number of CSPs prepared in iv rooms daily in the United States is unknown, at least to me, but has to be somewhere in the neighborhood of a million. (2) Combine that with published literature that puts sterile compounding errors around 11%, (3) and that’s some scary stuff. With numbers like these, I wonder how many mistakes make their way to the patient?
The iv room is a busy place with a lot of dangerous medications. It’s also a place where a lot of errors occur. Â With the availability of commercially available products that can easily prevent these types of errors, there’s really no excuse for continuing to use a completely manual process.
———————
(1) Syringe pull-back method is when the empty syringe used for each drug or electrolyte is left alongside the item with its plunger pulled back to the volume that was added. The pharmacist looks at the empty syringe with plunger pulled back and compares volume to the volume necessary to accurately prepare the CSP. This is common practice in many pharmacies even though it has been declared unsafe. I continue to be surprised that pharmacies use the syringe pull-back method.
(2)Â Using a number of 1.5 CSPs per patient, per day in acute care hospitals, and using 795,603 licensed Community Hospital beds in the United States (1999 – 2013 AHA Annual Survey, Copyright 2015 by Health Forum, LLC, an affiliate of the American Hospital Association), the number of CSPs produced per day in the United States exceeds 1 Million.
(3)Â Am J Hosp Pharm 1997;54:904-912
Leave a Reply