I wrote about the NEPS labeling solution for pharmacy way back in May of 2009. The product basically extends the functionality of the pharmacy information system by giving users the ability to print custom labels for medications through the use of different fonts, colors, and images. It’s well thought of in certain pharmacy circles. In the hands of the right people NEPS can be an effective way to create some pretty cool labels. In the hands of others it’s a good way to create confusion.
(more…)
Category: Pharmacy Practice
-
Quick Hit: Thoughts on NEPS labeling solution for pharmacy
-
Getting creative with pharmacy labels: dosing calculations
I was searching for inpatient pharmacy label examples, specifically IV label examples, for a project that I’m working on and came across a site called RxLabelToolkit.com. It’s a neat little site that offers quite a bit of information on label design. I don’t know if the business is still active as the most recent post I can find on their blog is from December, but it’s worth a few minutes of your time to stop and have a look.
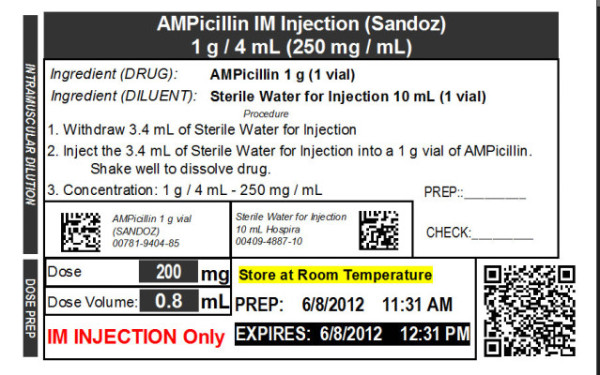
RxLabelToolkit.com: “One of the most valuable features of BarTender for pharmacy, is the ability to perform pharmaceutical calculations right within the label application. This allows us to build a label that can calculate a dose, an infusion rate, expiration date or a taper schedule. Any mathematical formula needed can be performed right in the label application.â€
The site has some pretty cool examples. The ampicillin label below is my favorite. There’s also a brief slide presentation that walks you through all the fields on the example label.
-
The future of 340B, my perspective
The snippets below are taken from a recent article in Pharmacy Times: The Future of 340B: It’s All About Perspective
“Established more than 20 years ago [the 340B Drug Discount Program], this legislation was enacted to assist different health care settings in providing excellent care for indigent and vulnerable patients. To allow this to happen, safety net providers have access to discounted outpatient drugs from manufacturers. By being able to purchase the discounted medications, these qualifying organizations are able to utilize the savings to provide care for those uninsured and underinsured patients. “ – The 340B Drug Discount Program can be a great thing for healthcare systems that care for a lot of ‘uninsured’ or ‘underinsured’ patients. These are often time indigent patients.
(more…) -
Please take this short online pharmacokinetics survey (5 minutes)
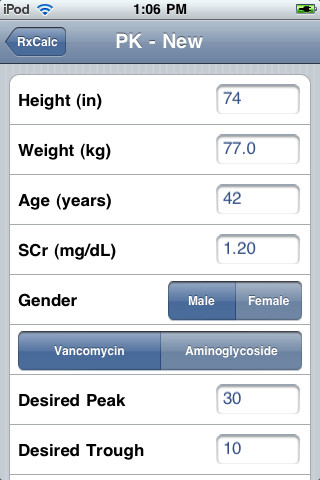
Several years ago my brother and I designed and developed RxCalc, a pharmacokinetics calculator for the iPhone and iPod Touch. It has been several years since we’ve updated the application, but we’re hoping to change that.
Below is a short survey that will help us determine what features and functions healthcare professionals would like to see in their pharmacokinetics application. The survey is short, but will provide us with important information. Please take a few minutes to complete the survey and submit your response.
-
What’s the single most important technology introduced into pharmacy operations in last 10 years?
I asked this question on Twitter today looking for opinions from the countless number of people roaming the internet. Alas, I received not a single response. Not one. I’m starting to think that Twitter, and most other social media, is worthless as a way of gathering information from people. Oh sure, my Twitter feed is great for consuming an endless string of articles and links, but the few times I’ve actually reached out to the Twittersphere with a question I’ve ended up with bupkis.
(more…) -
Motion sensing technology in the IV room
I’ve always been intrigued by motion sensing technology like Microsoft’s Kinect for the Xbox system. My interest was rekindled last week when I came across an article at Fast Company taking about Kinect Hacks.  I do what I always do when I read something interesting, I Tweet about it.
I still think Kinect would be cool in a pharmacy IV room – Five Amazing Hacks That Make Us Giddy For The New Kinect http://t.co/NOYurxQfJO
— Jerry Fahrni (@JFahrni) August 10, 2013
-
Crowdsourcing pharmacokinetic data
 Pharmacokinetics is something that every hospital pharmacist is intimately familiar with. It just so happens to be one of the things that physicians routinely ask pharmacist to handle. It’s not that doing pharmacokinetic (PK) calculations is difficult, but crunching the numbers can be time consuming and there are occasional traps that can lead to problems for those not experienced in such things.
Pharmacokinetics is something that every hospital pharmacist is intimately familiar with. It just so happens to be one of the things that physicians routinely ask pharmacist to handle. It’s not that doing pharmacokinetic (PK) calculations is difficult, but crunching the numbers can be time consuming and there are occasional traps that can lead to problems for those not experienced in such things.I’ve performed literally thousands of PK calculations* during my career. When I first began practicing pharmacy there were lots of drugs that required pharmacokinetic monitoring: lidocaine, procainamide, vancomycin, the aminoglycosides, phenytoin, digoxin, phenobarbital, among others. Over the years many of these drugs have been replaced by newer, better agents or simply fallen out of favor.
Some PK calculations can be harder than others, like phenytoin because of its reliance on Michaelis-Menten parameters, or lidocaine because it required loading doses due to its multi-compartment distribution. But others are brain-dead simple. Vancomycin is like that. A monkey could do a new vancomycin start.
During those years one thing remained constant; to perform PK calculations all you needed was a pencil and a calculator. Things have changed over the years with the increased use of computerized software and mobile devices, but the nuts and bolts of the process remains the same.
With the advent of big data one has to wonder why pharmacists continue to do this. Is it a matter of tradition that keeps us tied to pharmacokinetics? It’s hard to say. I remember looking at population trends when I was working as a critical care pharmacist nearly ten years ago. Another pharmacist, Patrick and I kept a spreadsheet of patient ages, gender, height, weight, renal function, infection site, infectious organism(s), and of course drug levels. We were attempting to use our data to find trends that would help us initiate therapy more accurately. Our project never really panned out. We discovered very little in the year we collected the information. The reason for our failure was lack of data and our inability to rigorously study the information in front of us. That’s no longer the case. Given the opportunity, data scientists could analyze hundreds of thousands of PK starts and adjustments to uncover things that Patrick and I could have only dreamt of a decade ago.
So one has to ask whether or not this is being done today, and if not why?
—————————————————-
*conservatively I see it as follows:
10 years as a “clinical pharmacistâ€
50 weeks per year working (hey, everyone needs a vacation)
average of 6-10 new PK starts per day; twice that number of monitoring
taking the low road: 10 x 50 x 6 = 3000 -
Pharmacist remote order verification, i.e. checking something from afar
The current pharmacy practice model utilizes pharmacists to check everything that leaves the pharmacy. Right or wrong that’s the way it is. I don’t think it’s necessary, but I’m not the guy in charge of such things.
Pharmacy has tools to help get pharmacists out of the physical pharmacy, namely tech-check-tech and remote order verification, but I don’t see such things used with consistency. My position on tech-check-tech is well documented; it’s underutilized. Using technicians “at the top of their license” would go a long way in freeing up pharmacists to do other things. The problem at the moment is that many pharmacists don’t want to relinquish the “final check” responsibilities. It’s silly, but true.
(more…)