I’ve written about the need for better integration and interoperability before. I’ve even written about the trend toward integrated systems. In January 2014, I wrote that “healthcare systems, and more specifically pharmacies, have started to understand the importance of having integrated systems.â€
Here we are two years later, and to my surprise, we seem to be making great progress. There are obvious trends appearing in pharmacy.
While walking through the Exhibit Hall at ASHP Midyear, it was clear that integration was on the minds of many – people, healthcare systems, vendors. The term “integration†was being thrown around like confetti at Mardi Gras.
Companies like Baxter, Omnicell, and Aesynt are making a concerted effort to improve integration, each using a different approach. Baxter has a new EPIC interface, allowing DoseEdge to feed information directly into the EHR. Omnicell has made significant strides in creating a centralized database across their inventory management products for the central pharmacy. Aesynt is focusing on pulling data from several disparate sources for their data analytics tools, REINVENT and Formulary Tool Kit (FTK)
Acquisitions continue to be on everyone’s mind. Aesynt recently became part of Omnicell, and CareFusion is part of BD. Others are possible by year’s end.
Pharmacies want fewer disparate systems and are willing to sacrifice functionality for integration. I won’t go into specifics here, but several pharmacies that I’ve spoken with are opting for systems that are, in my opinion, missing key components, in favor of integration with their EHR or another system.
Looking over the landscape, it’s obvious that integration of systems will no longer be optional. The big boys are all in, and the little guys should take note as to not be left out in the cold.
Whether or not future editions of USP General Chapter <797> will include recommendations for IV room automation and technology is a great question, and one that I’ve been pondering for quite some time. I’m torn as to whether or not I think adding such recommendations to a USP General Chapter is a good idea.
On one hand, I believe that pharmacy is over-regulated as it is. The amount of time spent by pharmacy personnel adhering to and documenting compliance to regulations currently in place is staggering. New regulations are frequently added to the process, but rarely, if ever taken away.
On the other hand, pharmacies refuse to utilize game-changing automation and technology even when they know it has the potential to improve operations, improve patient safety, and decrease cost. I’ve met many pharmacy directors and operations managers over the years that operate in a state of willful blindness when it comes to adoption of technology in the pharmacy.
While I don’t support adding, even more, regulatory requirements to pharmacy practice, I’m in favor of increased use of pharmacy automation and technology, especially in the IV room. It’s a conundrum.
With that said, it may become a moot point as it is possible that recommendations addressing the use of iv room automation and technology will find their way into the next revision of USP General Chapter <797> Pharmaceutical Compounding—Sterile Preparations. Recent discussions with people close to the situation lead me to believe it could happen.
Should that occur, it would likely be a good thing for pharmacy practice in the long run as it would drive adoption of CSP preparation technology. Even if the Expert Compounding Committee were to recommend adoption and not mandate it, i.e. “should†versus “shallâ€, the industry would surely take note. Recommendations that show up in <797> have a way of trickling down into other regulatory agencies as well as into the minds of inspectors and pharmacy directors. For example, the 2015 California Lawbook for Pharmacy(1) states that “The board shall review any formal revision to General Chapter 797 of the United States Pharmacopeia and The National Formulary (USP–NF), relating to the compounding of sterile preparations, not later than 90 days after the revision becomes official, to determine whether amendments are necessaryâ€. Regardless of whether or not the board takes action, they are sure to take notice.
It’s too early to say whether or not the revisions to Chapter <797>Â will include recommendations for CSP preparation technology, but I suspect we won’t have to wait long to find out. Chapter <797> is currently up for public comment until January 31, 2016. Based on recent changes to USP General Chapter <800>, I suspect revisions to Chapter <797> will become official in a similar timeframe so that the chapters can be properly harmonized. Only time will tell.
Jerry talks about his experience with Virtual Reality and where there may be some potential for use in pharmacy.
Show Notes:
Host: Jerry Fahnri, Pharm.D.
0:00 Introduction 0:28 My experience with VR 1:59 VR tiers and products 5:05 Application of VR – General 5:50 Application of VR – Healthcare 7:51 Application of VR – Pharmacy 13:01 Application of VR – Vendors
Recently a friend and colleague reached out to me looking for guidance on published studies showing positive ROI for IV room automation and technology. There’s precious little literature covering this practice are of pharmacy, much less getting into things like ROI.
Why is that? As I see it, the problem comes down to these three things:
Bias. Some of what is written, especially in the “throw-away journals†is sponsored content, and as a result, presents a lop-sided view to the reader. It’s still worth reading, but always with a grain of salt.
One-size fits all. Nope. There are too many approaches to compounded sterile product (CSP) production in pharmacies across the U.S. I’ve been in more than 20 acute care pharmacies over the past few years looking at operations, and it’s clear that we’re all doing exactly the same thing completely differently. The solution for a 200-bed community hospital may or may not be a good fit for a 600-bed level 1 trauma center, or a healthcare system with centralized IV admixture servicing several facilities. It all depends on your needs. One must look at several variables and the specific needs of the pharmacy, patient, and healthcare system. Doing anything less is a recipe for wasted time, energy, and resources.
Traditional literaturedoesn’t work. The typical literature cycle doesn’t work for pharmacy technology. Even though pharmacy automation and technology moves slowly, it still changes at a much more rapid pace than therapeutics and/or best practices. Changes in clinical approaches to the use of medication takes time, and once established typically last until something better comes along. We’re talking years here, sometimes decades. That doesn’t work for pharmacy automation and technology. Research on an IV room robot that was purchased in 2009, installed in 2010, and published about in 2015(1) is of little use to pharmacists looking for relevant information in 2016. It’s doubtful that the technology is still in a form today that could be easily compared to that presented in the article. It’s also entirely likely that the product no longer exists. An article like that offers little to those considering investing in pharmacy automation and technology, perhaps except for general interest or curiosity.
There is clearly a lack of literature on the subject, but there is also clearly no one size fits all approach. If you’re truly looking for the best way to implement automation and technology in your pharmacy, I recommend the following:
Go ahead and do a literature search, focusing on the “throw-awaysâ€. I know, I just spent a page telling you this doesn’t work. You won’t find enough to make a decision, but it will, at least, give you an idea of what products are on the market.
Get some boots on the ground. There is no substitute for seeing the technology in action. Go visit people that are using the product. Don’t be cheap. If you’re going to drop a million dollars on a compounding robot, be willing to spend some money traveling around and looking at these things in real-world environments.
Take your time. This is one area where making a snap decision will cost you. Not only will you spend resources on something that might not be the best fit, you’re likely to be stuck with it for a while.
If you can’t do the above yourself, hire a consultant. Sounds a bit self-serving, but it’s true. Consultants will cost you upfront, but will save you several-fold the cost in the long run.
—————————————————
Nurgat, Z., Faris, D., Mominah, M., Vibar, A., Al-Jazairi, A., Ewing, S., … Al-Jedai, A. (2015). A three-year study of a first-generation chemotherapy-compounding robot. American Journal of Health-System Pharmacy, 72(12), 1036–1045. http://doi.org/10.2146/ajhp140256
Several years ago there was a group of pharmacists taking a serious look at the long-time practice of having pharmacists review virtually all drug orders, sometimes referred to as nearly universal prospective order review (NUPOR). The argument for NUPOR is that it is needed to ensure complete, accurate orders. The argument against NUPOR is that it’s expensive, time-consuming, and unnecessary in many instances. I fall into the latter category of pharmacists, i.e. NUPOR is an antiquated practice that needs to be done away with.
There are those that argue that doing away with NUPOR is dangerous and removes the pharmacist from the medication use process. Nothing could be further from the truth. By making NUPOR a requirement you have taken pharmacists out of the healthcare discussion. NUPORÂ forces pharmacists to be tied to a terminal when they could be doing other things.Â
The introduction of Electronic Health Records (EHRs) and Computerized Provider Order Entry (CPOE) have created a perfect opportunity to change the concept of NUPOR.
Here are some scenarios to think about:
Setting, a large acute care hospital with a busy Emergency Department (ED). Physicians frequently order boluses of NS, or other fluid. Does a 1L bolus of NS ordered for an adult patient in the ED really require verification by a pharmacist prior to administration? Ask yourself, as a pharmacist, what set of circumstances would cause you to reject such an order and call the physician?
Setting, hospital OB-GYN unit. Adult patient comes in for delivery. Physician orders 50 mg of IV meperidine x1 for pain. The patient is in good health, labs are normal, and has no allergies to the medication. Is there any reason that such an order needs verification? What would cause you to reject it and call the physician?
Setting, general medicine floor of a hospital. Elderly patient admitted following a minor surgical procedure. The patient is experiencing constipation secondary to the procedure and medication for pain. Physician orders a bisacodyl suppository or MOM x1 to help get things moving. Labs are ok, the patient has no allergies to the medication, and there are no significant drug interactions. Is there any reason that such an order would require a pharmacist’s blessing?
The list goes on and on. I suppose one could argue that there could be potential for a physician to blow through a catastrophic problem with the drug order that would harm the patient. Sure, that could happen. However, I would argue that a good system would allow the healthcare system to place hard stops in places where there is genuine concern or potential for a problem.
I just don’t see NUPOR as necessary in today’s healthcare environment, especially for those healthcare systems using EHRs and CPOE. Don’t agree? That’s cool. Use the comment section below to convince me I’m wrong, but make sure you have a good reason, because if you don’t, I’ll mock you in front of the other children.Â
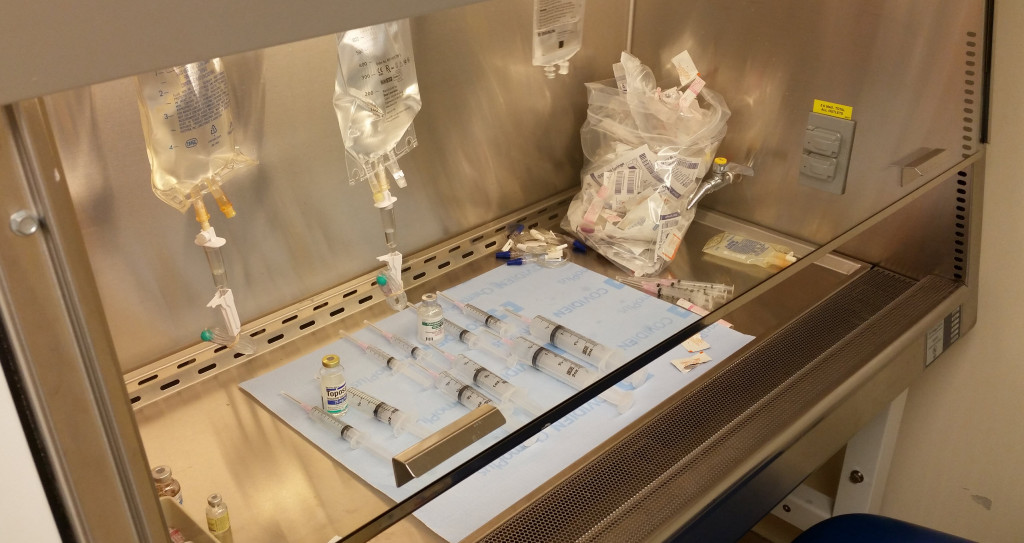
I spent a short time observing iv preparation in two separate, distinctly different pharmacy environments in the weeks leading up to the new year.
One was a traditional iv room in a large acute care pharmacy with multiple pharmacy technicians and pharmacists putting out hundreds of compounded sterile preparations (CSPs) per day. The second was a segregated compounding area in a satellite pharmacy with one pharmacy technician and one pharmacist using a glove box to prepare STAT and first dose CSPs to critical care areas.
Neither area utilized technology for CSP preparation, instead opting for the good ole fashioned syringe pull-back method (1). In the case of the traditional iv room, I observed instances of up to twenty different CSPs with empty vials and syringes laid out awaiting pharmacist verification. In the segregated compounding area with glove box, CSPs were typically prepared one at a time or in small batches.
During my short time observing CSP preparation in the two areas I witnessed errors that would have easily been caught with the use of readily available technology. Â Here are two examples:
Wrong drug selection – This may be the most common error seen in iv rooms. In this particular case, the technician used a vial of potassium phosphate (KPhos) for a CSP that called for sodium phosphate (NaPhos). The use of bar code scanning for verification during the compounding process would have prevented this error.
Calculation error resulting in an incorrect dilution – A patient-specific order called for 20 mg of hydrocortisone in a total volume of 2 mL to be placed in a syringe for iv administration. The technician started by first making a stock hydrocortisone syringe from which to draw the dose. This is a common practice. The resulting stock syringe should have contained 100 mg of hydrocortisone in 10 mL of solution, i.e. final concentration of 10 mg/mL. Instead, the technician calculated the final volume as 25 mL, resulting in a final concentration of 4 mg/mL in the stock syringe. So when the patient-specific dose of 2 mL was drawn into the syringe the final dose was only 8 mg. The pharmacist almost let it go, but something made him take a second look. It was only when he asked the technician to explain the process that the error was discovered. The use of bar code scanning for verification during the compounding process would not have prevented this error. But, the use of step-by-step instructions with intermediary step checks during the stock syringe prep, or the use of gravimetrics, would have.
The number of CSPs prepared in iv rooms daily in the United States is unknown, at least to me, but has to be somewhere in the neighborhood of a million. (2) Combine that with published literature that puts sterile compounding errors around 11%, (3) and that’s some scary stuff. With numbers like these, I wonder how many mistakes make their way to the patient?
The iv room is a busy place with a lot of dangerous medications. It’s also a place where a lot of errors occur. Â With the availability of commercially available products that can easily prevent these types of errors, there’s really no excuse for continuing to use a completely manual process.
———————
(1) Syringe pull-back method is when the empty syringe used for each drug or electrolyte is left alongside the item with its plunger pulled back to the volume that was added. The pharmacist looks at the empty syringe with plunger pulled back and compares volume to the volume necessary to accurately prepare the CSP. This is common practice in many pharmacies even though it has been declared unsafe. I continue to be surprised that pharmacies use the syringe pull-back method.
(2)Â Using a number of 1.5 CSPs per patient, per day in acute care hospitals, and using 795,603 licensed Community Hospital beds in the United States (1999 – 2013 AHA Annual Survey, Copyright 2015 by Health Forum, LLC, an affiliate of the American Hospital Association), the number of CSPs produced per day in the United States exceeds 1 Million.
I’m sure that most of you are aware, but just in case, I thought I would pass this little tidbit along.
The Compounding Expert Committee announced on November 20, 2015, that USP has approved a new General Chapter USP <800> – Hazardous Drugs—Handling in Healthcare Settings. The revised chapter will be published February 1, 2016, in the first supplement to USP 39-NF 34. USP standards typically become official 6 months after publication, but the Expert Committee approved a delayed official implementation date of July 1, 2018 to prevent any undue hardship on systems that need to make major changes.
You can get more information on General Chapter <800> Hazardous Drugs—Handling in Healthcare Settings to be Published in USP 39–NF 34, First Supplement here.
This year’s ASHP Midyear Clinical Meeting was held at the Ernest N. Morial Convention Center in New Orleans, Louisiana on December 6 through December 10, 2015. For many, the Midyear Meeting is about the latest in clinical advances, but for me, it’s an opportunity to see all the new pharmacy automation and technology. And the best place to see the latest and greatest technology is in the exhibit hall.
Below you will find my thoughts on what I saw while roaming the exhibit hall. By no means is this an exhaustive list, but rather items that I think are worth mentioning and thinking about.
PHARMACY CLEAN ROOM
“Sterile compounding is a significant but perilous core pharmacy process in dire need of improvement.†– ISMP Jan 2015
The pharmacy clean room (a.k.a. iv room) continues to get a lot of attention, and rightly so. With the introduction of USP Chapter <800> and proposed changes to USP Chapter <797>, the clean room is on everyone’s mind. This year’s exhibit hall was a direct reflection of this.
The clean room automation and technology space is It was bound to happen. Over the past few years, several vendors have introduced products designed to help pharmacists with compounding sterile products or meeting clean room regulatory requirements.
Aesynt is now part of Omnicell and CareFusion is part of BD. BD has had more time to ramp up their messaging and it was obvious in their exhibit this year.
The Plus Delta Technologies booth was empty. Plus Delta’s products include PD, a medication tracking system, and IVTtrac, a semi-automated iv workflow management system. It is unclear whether the company has been sold, has gone belly up, or is simply keeping a low profile
APOTECA was not present in the Midyear Exhibit Hall this year. If you recall, APOTECA is the company responsible for APOTECAchemo, a robot for compounding hazardous drugs. Last year about this time they introduced APOTECAps, a semi-automated iv workflow management system. The company was conspicuously absent.
There was a good number of booths offering clean room consulting. More than I’ve seen in past years.
Aesynt – previously McKesson Automation, now part of Omnicell – was focused on data analytics in the clean room with two new products: REINVENT and Formulary Tool Kit (FTK). I wrote about REINVENT after the ASHP Summer Meeting in Denver. FTK is a tool designed to help pharmacies extend BUD in the cleanroom.
BD and Baxter seem to be running parallel races. Baxter had a press release at the meeting that focused on DoseEdgeBD did the same for Cato. Baxter will be pushing their Epic integration in the coming year.
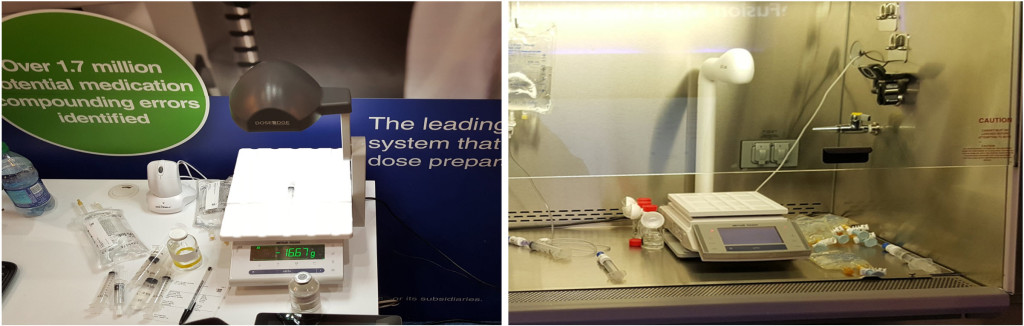
Baxter was showing off their DoseEdge scales for the first time ever at a Midyear event. DoseEdge has had gravimetric functionality for quite some time, but the concept has never been popular with their customers. Apparently that has all changed. Based on conversations with insiders, this appears to be a direct result of pressure from BD’s gravimetric-centric approach.
Imaging platform and scales from DoseEdge (left) and BD Cato (right)
MedKeeper showed off a new booth at Midyear with Verification front and center. Verification is MedKeeper’s semi-automated iv workflow management system. Something that caught my eye while I was in the MedKeeper booth was the images captured by Verification. They’re really quite good. I was especially surprised to find that some of the images I was looking at were taken from outside an isolator. That’s right, the device was mounted outside the isolator, thus limiting the hardware in the hood.
Verification by MedKeeper – images shown on screen taken from outside an isolator
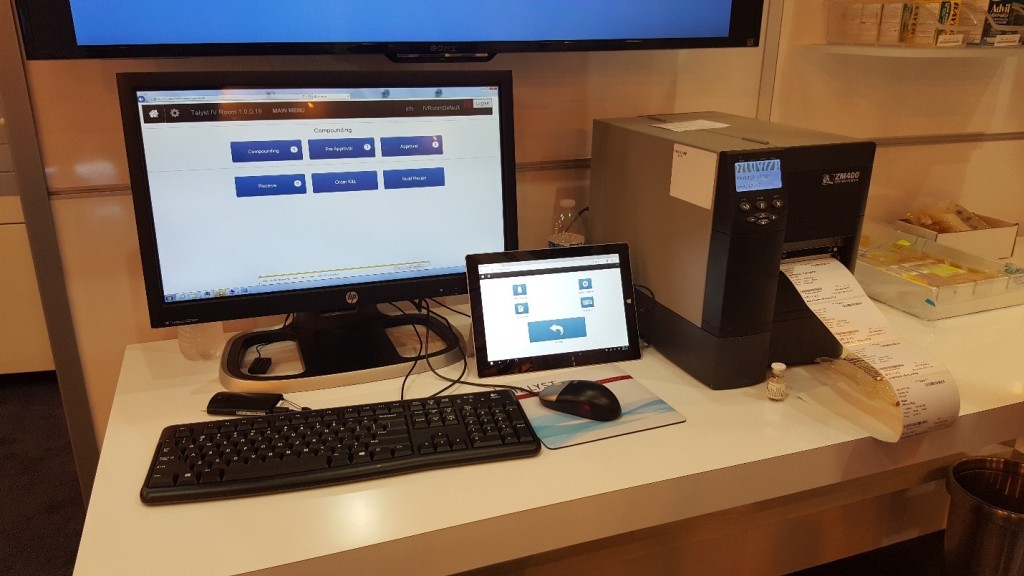
Talyst had Talyst IV Room on display. Talyst IV Room is part of the company’s mobile inventory management solution and offers users the ability to build IV kits utilizing barcode scanning for verification, as well as the ability to track sterile preparations throughout the compounding process.
Talyst IV Room product on display
Grifols introduced a new hazardous drug compounding hybrid robot, Kiro Oncology. Kiro is a bit different from previous robots as it uses two robotic arms to compound sterile preparations. It’s an interesting concept.
Kiro Oncology robot from Grifols
Compounding robots were out in full force: Aesynt with v.STATION, ARxIUM with RIVA, and Grifols with Kiro Oncology.
RFID-ENABLED TECHNOLOGY
RFID-enabled technology was more prevalent at this year’s ASHP Midyear than I can recall in previous years. Booths that had RFID-enabled products on display were typically busy, and the people in those booths were engaged in conversation.
Does this mean that pharmacy has finally turned the corner on RFID? Perhaps, but the technology still has some barriers, both real and perceived to overcome. It is clear to me, however, that RFID has niches in pharmacy and vendors are finding those niches.
Three booths that I thought were particularly busy were MEPS Real-Time, Inc., Kit Check and FFF Enterprises.
MEPS Real-Time, Inc. was showing off their Intelliguard RFID system, which includes an RFID-enabled medication tray management system, controlled temperature cabinets (CTCs) – both refrigerated and room temperature – and a virtual logbook for tracking medication trays.
Kit Check had their “Little Blue Box†scanning station in the booth, which is part of their RFID-enabled medication tray management system. In addition, Kit Check was showing off their RFID-enabled Anesthesia Check system, which I thought was pretty cool. The design is well thought out and offers some nice functionality.
FFF Enterprises is a distributor of plasma products, vaccines, biopharmaceuticals, and biosimilars. Part of their product line includes Verified Inventory Program-Consignment (VIPc), which includes RFID-enabled refrigerators that offer automatic track and replenishment for their product line. Cardinal Health does something similar.
SencorpWhite was on hand with a small booth providing information on their RFID capable carousels. They didn’t have a physical carousel in the booth as in previous years, but instead opted for literature and a looping video to support their product offering.
PharMEDium announced that they will be making pre-filled syringes with RFID tags embedded in the labels. This is big, but the announcement went unnoticed by many. I wouldn’t have known about the move had I not been speaking to one of the vendors mentioned above. I verified this with one of the PharMEDium executives and was informed that the RFID-enabled pre-filled syringes will not be proprietary to any single company, and will be made available to anyone looking for pre-filled syringes with embedded RFID tags.
COLD CHAIN TECHNOLOGY
It has been clear for quite some time that refrigeration is going to be important for the next generation of pharmaceuticals, including biologicals. Pharmacies will need to invest in and utilize better security, as well as real-time monitoring for temperature, humidity, and inventory.
The exhibit hall was full of vendors offering real-time monitoring. Have a data connection, i.e. “the internet� If so, then you have everything you need to use many of these systems. Vendors are offering cloud-based storage of information, which means anytime, anywhere access to data. Real-time monitoring and alerts mean that pharmacy directors will have peace of mind that their pricey inventory is in date, properly stored, and in stock. It’s a win-win.
All the major pharmaceutical grade refrigerator vendors had a presence in the exhibit hall: Helmer, Follett, Migali Scientific. Not to mention seeing many other vendors with one of these brands in their booth. Partnerships and alliances appear to be the most efficient method of ensuring that you can offer a refrigerated solution to your customers.
Some items that I felt were particularly interesting in the cold chain area:
RFID-enabled refrigerators. See the section on RFID for more detail.
The Evolve line of pharmacy-grade refrigerators from Phononic were quite impressive. These refrigerators are powered by SilverCoreâ„¢ Technology. They have no compressor, meaning they have no mechanical parts, run quiet, use less electricity, and generate less heat. The refrigerators use solid-state heat pump technology coupled with a non-hazardous, non-toxic refrigerant. In addition, the units provide alerts for temperature, door, battery, memory, loss of Wi-Fi, and loss of power. Check the image below showing the solid-state “pumpâ€.
Phononic compressor-free refrigeration technology
Vaccine Smart-Fridge. I wrote about this back in September. The Smart-Fridge is an interesting concept. The system offers single-point access to vaccines, providing real-time alerts on inventory shortages and temperature. Automated temperature monitoring ensures that things stay within their appropriate temperature range, and analytics and historical dispensing data are collected and made available to the user.
STRIP PACKAGING FOR AMBULATORY CARE
Strip packagers have been around for a long time. They were popular in acute care for a while, but not so much anymore. However, there appears to be renewed interest in the technology for use in ambulatory care pharmacy, especially as a method of improving medication adherence. I spoke to several strip packaging vendors that are seeing renewed interest in the technology. Most attribute this to the introduction of strip packaging as a medication adherence platform made popular by recent coverage of PillPack.
DYNALABS DVxâ„¢ Onsite Drug Verification System. DVx allows users to quickly and easily verify drug identity and strength (concentration) in real-time. The demo was impressive. The representative that I spoke with said that DYNALABS currently had a limited reference library, but were adding new drugs all the time.
ScriptCenter by Asteres. Think of ScriptCenter as something similar to the Amazon Locker model. Pharmacies fill medications, place them in the ScriptCenter kiosk, and allow users to pick them up at their convenience. Kind of an ATM-style solution to medication refill pickup. The system sends messages to patients when their prescription is loaded and ready. Users can pay with credit card or payroll deduction. You can even load OTCs into ScriptCenter. I spoke to Dana Darger, Director of Pharmacy at Regional Health in Rapid City, SD about ScriptCenter. He has been using the unit to provide employees with 24/7 access to medication refills. So far he’s been pretty happy with the results. Dana commented that ScriptCenter has helped alleviate congestion in the outpatient pharmacy as well as give hospital employees easy access to their refills.
ScriptCenter by Asteres
Cactus Smart Sink. I wrote about the Cactus Smart Sink while attending Midyear. The Smart Sink is a pharmaceutical waste disposal container that renders its contents “unrecoverable, non-retrievable and unusableâ€. It’s small and unassuming. I thought it was pretty slick.
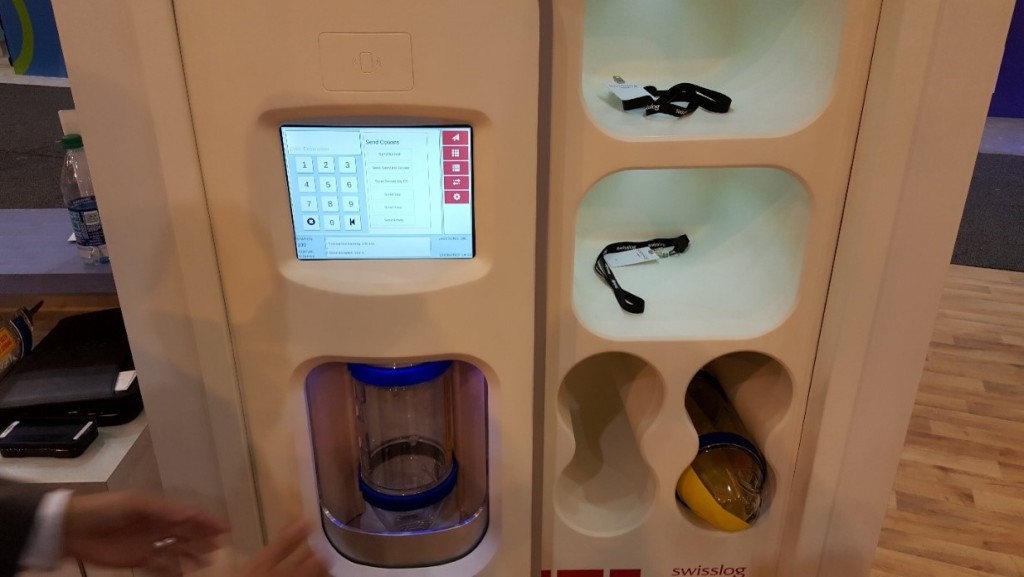
Swisslog Nexus Station. One has to wonder how a tube station can be exciting. Well, if you’ve ever worked in a pharmacy where items are queued up due to volume, then you’ll appreciate the Swisslog Nexus Station. The Nexus allows users to load up to five tubes at a time in a Lazy Susan-like configuration. Tubes can be loaded as non-secure or secure and the Nexus will keep track. Much more efficient than a “one-up†tube station.
Nexus Station by Swisslog
A PDF version of this report may be downloaded here.
Vestigo is web-based Investigational Drug Service (IDS) software made by the McCreadie Group, Inc., a privately held pharmacy software company out of Ann Arbor, Michigan. The McCredie Group is a small boutique company that builds software for niche markets like IDS.
I’ve worked in pharmacies that have an IDS, and let me just say that there’s a lot of record keeping involved and attention to detail is important. One would think that the “the drug†would be the most important thing, but that’s not really the case. Records, logs, and traceability are key.
Anyway, one of the products offered by the McCreadie Group is Vestigo. I’ve come across the product in pharmacies while traveling, but never really given it much attention. Because it’s such a niche product I couldn’t even tell you who they’re competing against.
Don’t go Googling for information on Vestigo, because you’re probably not going to find much. The company has done a pretty good job of not marketing their product and keeping relevant information off the internet. Not sure how that’s possible in this day and age, but I wasn’t able to find more than some old reference articles and press releases.
I have verified with the company that they will be at the 50thASHP Midyear Clinical Meeting and Exhibition in New Orleans in early December. I’m interested enough in the product to drop by their booth and have a look. Until then, here’s what the McCreadie Group site has to say about Vestigo:
Vestigo increases IDS safety and compliance…
Protocols structured in a logical and safe manner
Product selection limited to drugs used for the current protocol
Automated checks for expired products and IRB approvals
Patient management functions prevent dispensing to patients not enrolled
Accurate, electronic drug accountability records
High-quality, safe labels with barcodes
Built-in workflow for safe practices
Logging and audit trails required for HIPAA and 21 CFR Part 11 compliance
…and improves IDS efficiency and reduces costs
Electronic protocol managementFully automated protocol billing (increases revenue and reduces the cost of generating the bill
Electronic inventory management including tracking patient-specific items, returns and destructions
Reduced paperwork and handwriting
Integrated dispensing with automatic label generation
Extensive reporting to track operations, workload and financials
So if you’re in the market for an IDS solution, you might give Vestigo a look and request a demo.
EMR & EHR: “Of all the things that irrationally inflate health costs, one of the top concerns is people who just don’t take their prescribed medications. Medication adherence doesn’t sound like a high-tech issue, but a lot of interesting technologies are being thrown at the problem…. At the recent Connected Health Conference I talked to several companies taking on the difficult adherence problem from different angles. Medisafe aids patients in self-monitoring, Insightfil creates convenient packaging that groups pills the ways patients take them, and Dose doles out medication at prescribed times.† – The author goes on to describe some of the technology. The content is worth a few minutes of your time.
Here’s the thing, technology may not be the solution.
@JFahrni or we could take the time & explain to pts how to/importance of taking their meds. Not sure these solve the root issue
There’s no question that medication adherence is a problem. How big is the problem? Well, according to an article in The American Journal of Medicine, 28% of new prescriptions never get filled, and among patients who do fill their prescriptions, adherence rates are less than 50%. The New England Healthcare Institute NEHI in 2009 [PDF] estimated that the cost of non-adherence was about $290 billion annually. It’s probably well over $300 billion now, but the number I see in most presentations is $290 billion. Hey, it’s a good, scary number.
Medication adherence, or non-adherence as the case may be, not only complicates things for patients but for the entire healthcare system.
The problem is well defined, i.e. people aren’t taking their medications properly, but the solution has eluded healthcare for a long time. That’s likely because the reasons for non-adherence vary widely and have been debated and discussed as long as I’ve been a pharmacist. Have we made progress? It’s hard to say. I suppose it all depends on your definition of progress. We have lots of medication adherence tools at our disposal; reminder systems, mobile applications, smart medication organizers, alert systems for medication bottles, and so on. I suppose that could be considered progress.
All these toys have a place in medication adherence, but the fundamental problem goes well beyond their scope. Medication adherence is a multi-faceted problem with roots in psychological behavior, socioeconomic background, and demographics.
However, one thing that people seem to overlook is that the contact point for most patients and their medications is a pharmacist. According to a recent report published by the National Community Pharmacy Association (NCPA), “the biggest predictor of medication adherence was patients’ personal connection (or lack thereof) with a pharmacist or pharmacy staff.â€
A patient’s introduction to medication use should begin by developing a relationship with a pharmacist at the point of care, whether that’s a hospital or a community pharmacy. In hospitals, patients should speak with a pharmacist upon admission, and again upon discharge. No patient should ever leave the hospital without speaking to a pharmacist or without medications in hand.
This is an oft-overlooked opportunity within healthcare systems. For hospitals that don’t have the resources to speak with every incoming and outgoing patient, look to your local community pharmacies. Find community pharmacies in the area that are willing to partner with the healthcare system to provide bedside medication delivery and consultation, thus beginning the process of building a working relationship between patient and pharmacist. As the patient moves from the hospital back into their daily routine, the relationship with their pharmacist will continue to grow. The payoffs are huge, especially for those patients with chronic diseases like diabetes, asthma, hypertension, hypercholesterolemia, and so on.
Not all patients are willing or able to be compliant, but some are, and those are the ones we hope to reach. Using a cost for non-adherence of $300 billion annually, a conservative positive impact of 10% could add up to more than #30 billion a year in savings, not to mention the positive impact on a patient’s quality of life.
Bottom line, get a pharmacist involved early and often. Medication adherence, it’s what we do.